Weight loss surgery has certainly evolved…thank goodness! Don’t get me wrong, it is not without any risk but the procedures available today are much safer and more effective than procedures of the past.
This overview includes the three primary surgical procedures performed within the United States as of the publication of this book along with the advantages, risks and typical results/outcomes for each. These three procedures are the Sleeve Gastrectomy (also referred to as the Gastric Sleeve), the Laparoscopic Adjustable Gastric Banding (also referred to as LapBand® or Realize Band®) and the Laparoscopic Gastric Bypass.
Sleeve Gastrectomy:
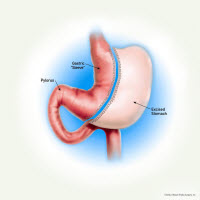 The Sleeve Gastrectomy is a newer laparoscopic weight loss surgical procedure in which a small “sleeve-shaped” stomach is created. Approximately 75% of the “stretchy” portion of the stomach is removed. This also removes the portion of the stomach that makes the hormone ghrelin. Ghrelin is a hormone which makes you feel hungry. The remaining “sleeve” of the stomach is about the size and shape of a medium banana. Because anatomy remains normal, this procedure can be considered for people with less weight to lose (50-60 lbs. overweight).
The Sleeve Gastrectomy is a newer laparoscopic weight loss surgical procedure in which a small “sleeve-shaped” stomach is created. Approximately 75% of the “stretchy” portion of the stomach is removed. This also removes the portion of the stomach that makes the hormone ghrelin. Ghrelin is a hormone which makes you feel hungry. The remaining “sleeve” of the stomach is about the size and shape of a medium banana. Because anatomy remains normal, this procedure can be considered for people with less weight to lose (50-60 lbs. overweight).
Advantages:
- The portion of the stomach that produces ghrelin (a hormone that stimulates hunger) is removed.
- The stomach is reduced in volume, but otherwise tends to function normally.
- No “Dumping Syndrome” since the pylorus is preserved.
- No intestine is bypassed so there is little chance of nutritional deficiencies.
- No implanted device that requires adjusting.
- Procedure is performed laparoscopically most of the time.
- Usually done as an outpatient.
This procedure tends to work due to 2 major reasons:
- You have a much smaller stomach and will feel full with eating only a small amount.
- There is a decrease in the hormone ghrelin so that hunger is much better controlled.
The sleeve gastrectomy was originally developed as the 1st stage of a 2 stage procedure (patients would undergo a conversion of the sleeve gastrectomy to a bypass procedure). However, it was found to work so well on its own that most patients did not need (or want) to go through with the next stage. This surgery cannot be reversed (i.e. once that part of the stomach is gone…it’s gone).
Risks:
Obesity, age, and other diseases increase your risks from any surgery. Below are identified risks related to surgery and the sleeve gastrectomy procedure based upon national averages? :
- Risk of death is 1:500-1,000
- Leaks (1-2%)
- Infection (2%)
- Blood Clot/Pulmonary Embolus (1%)
- Nausea/vomiting
- Peptic ulcer disease
- Formation of gallstones due to rapid weight loss
- Stricture (1%)
Some of these problems may require further surgical intervention
Typical Results and Outcomes:
Weight loss outcomes are tracked closely at the Center for Weight Loss Success. We are proud that outcomes here generally out-perform national averages. The average best weight loss for this procedure is 65-70% of a client’s excess body weight (i.e. if someone is 100 lbs. over their ideal body weight, average weight loss outcomes would be 65-70 lbs.).
A weight loss of only about 40% of excess body weight will often show significant improvement in many other medical problems:
- Many Type 2 diabetics will get off of their medications
- Hypertensive clients will have improvement or resolution of their hypertension
- Sleep apnea almost always improves
- Cholesterol improvement in most clients
- Arthritic symptoms improve
Laparoscopic Adjustable Gastric Banding (LapBand® or Realize Band®):
The FDA approved adjustable gastric banding surgery in June, 2001. However, it was developed in the 1980’s and has been used in Europe since 1993. In terms of surgical procedures for weight loss, this is the least invasive procedure.
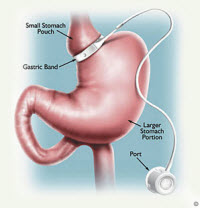 Laparoscopic adjustable gastric banding involves applying a band around the upper part of the stomach. As a result, this creates a small gastric pouch at the top of the stomach, with a small opening to the rest of the stomach. The band is made of an inflatable silastic ring that controls the flow of food from the small pouch to the rest of your digestive system. With this surgery, there is no cutting or stapling required dividing the stomach.
Laparoscopic adjustable gastric banding involves applying a band around the upper part of the stomach. As a result, this creates a small gastric pouch at the top of the stomach, with a small opening to the rest of the stomach. The band is made of an inflatable silastic ring that controls the flow of food from the small pouch to the rest of your digestive system. With this surgery, there is no cutting or stapling required dividing the stomach.
In addition to the band, a small port is connected by tubing to the inflatable ring around the stomach.
The port is secured just beneath the skin where fluid can be injected or withdrawn to inflate or deflate (adjust) the band. This results in increasing or decreasing the size of the opening between the upper small gastric pouch and the lower portion of the stomach. The need for an adjustment is determined by the surgeon based upon weight loss and symptoms related to eating.
Like any tool, it can be used correctly or incorrectly. Used incorrectly (such as drinking high calorie liquids) you will have relatively poor weight loss or even weight gain. It is still diet, exercise, and behavior change which produce weight loss. Thus, following your surgeon’s recommendations is crucial to your overall success.
Advantages:
The advantages cited in the literature are outlined below:
- Risk of death is approximately 1:1000
- There is no division or re-routing of intestinal tract
- Minimal risk of malnutrition
- The procedure is considered reversible since the Band can be removed with minimally invasive technique if needed
The band is adjustable:
- Often performed under fluoroscopic guidance
- May require 4-6 adjustments during the first year (or more)
- Adjustments need to be checked yearly – forever
The band is effective with the following considerations:
- Weight loss success is directly related to:
- close clinical follow-up
- appropriate adjustments
- exercise
- diet and behavior modification
The potential disadvantages of laparoscopic adjustable gastric banding are as follows:
- Weight loss is typically slower when compared to other weight loss surgeries
- Adjustments are required throughout your lifetime
- Problems can develop secondary to the mechanical device (see Risks)
Risks:
Obesity, age, and other diseases increase your risks from any surgery. Below are identified risks related to surgery and the laparoscopic adjustable gastric banding procedure based upon national averages.
- Risk of death is 1:1000
- Infection (<1%)
- Blood Clot/Pulmonary Embolus (1%)
- Gastric pouch dilation potentially requiring further surgery (5%)
- Band slippage or migration often requiring further surgery (5%)
- Band erosion requiring further surgery for band removal (1%)
- Access port problem or tubing leak requiring further surgery
- Nausea/vomiting
- Peptic ulcer disease
- Formation of gallstones due to rapid weight loss
Some of these problems may require further surgical intervention
Typical Results and Outcomes:
Following are expected results and outcomes based upon national averages:
- Average weight loss is 45-50% of excess body weight, but with aggressive diet and exercise changes you can lose almost all of your excess weight.
- A weight loss of only about 40% of excess body weight will often show significant improvement in many other medical problems:
- Many of Type 2 diabetics will get off of medications
- Hypertensive clients will have improvement or resolution of their hypertension
- Sleep apnea almost always improves
- Cholesterol improvement in most clients
- Arthritic symptoms improve
Laparoscopic Gastric Bypass Surgery
Laparoscopic Roux-en-Y Gastric Bypass was first originated by a group of Bariatric surgeons in California in 1994. This procedure is considered a combination procedure. It works by both restricting the amount of food consumed and also by providing some malabsorption. The surgical outcomes of this procedure seem to indicate that the weight loss results are similar to the traditional “open” procedure as long as the procedures are performed the same way.
The procedure begins by dividing the stomach to create a “pouch” that limits the amount of food that can be eaten. The pouch is about the size of one’s thumb and can hold about 20cc or 2-3 tablespoons of food. The larger excluded stomach, known as the gastric remnant, is stapled closed and separated from the pouch. This portion no longer receives food but has a normal blood supply thereby keeping it healthy.
The second step of the procedure involves taking a portion of the small intestine and creating a “bypass” or “Roux” limb that is connected to the new pouch to provide an outlet for food. This part of the procedure is what creates a slight malabsorption of nutrients to assist in weight loss.
The malabsorptive portion of the procedure also contributes to weight loss by causing a condition known as “Dumping Syndrome”. Most sugar consumed is normally absorbed in the first 1-2 feet of small intestine in normal situations. After the Gastric Bypass procedure sugar passes directly from the pouch into the lower small intestine. The unabsorbed sugar pulls fluid into the small intestine resulting in distension, increased motility (activity), cramping and a neurologic response that may cause an increase in heart rate, sweating, diarrhea, nausea, and even vomiting. Most patients will experience this at least once and will learn to avoid foods containing high sugar content, thus improving the chance for long-term weight loss success.
The following is a diagram of the described procedure: 
Risks:
- Possible conversion to an open procedure due to limited access and visibility
- There may be an increased risk for bowel obstruction in the long term
- Death (1:500-1,000)
- Pouch leaks – (1%)
- Deep venous thrombosis (1-2%)
- Pulmonary emboli (1%)
- Abdominal wall hernia (1%)
- Peptic ulcer disease (3-5%)
- Stricture (narrowing) at gastric pouch (1-2%)
- Small bowel obstruction (1-2%)
Typical Results and Outcomes:
The average best weight loss for this procedure is 70% of a person’s excess body weight (i.e. if someone is 100 lbs. over their ideal body weight, average weight loss outcomes would be 70 lbs.).
A weight loss of only about 40% of excess body weight will often show significant improvement in many other medical problems:
- Many Type 2 diabetics will get off of their medications
- Hypertensive clients will have improvement or resolution of their hypertension
- Sleep apnea almost always improves
- Cholesterol improvement in most clients
- Arthritic symptoms improve
Determining which procedure is right for you will require an evaluation with your surgeon and discussion about your specific situation. As you meet with him/her you will want to find out what their opinion is regarding the preferred weight loss procedure based upon your medical history as well as the number of procedures he/she has performed and their individual outcomes.
We invite you to view our Weight Loss Surgery webinar to learn more and decide if weight loss surgery is right for you: Weight Loss Surgery Webinar

Rhonda’s Opinion: The decision has to be yours but I am REALLY happy with the sleeve gastrectomy!





 Cat Keller has a wealth of experience in marketing, e-marketing, advertising and customer service and manages our Weight Loss Nutritional Store. She is always planning something fun and exciting. special events, discounts, giveaways – it’s never a dull moment. She is happy to help you with questions you may have regarding our products or services. Cat is a graduate of William & Mary, where she studied Government/Pre-Law and minored in Marketing.
Cat Keller has a wealth of experience in marketing, e-marketing, advertising and customer service and manages our Weight Loss Nutritional Store. She is always planning something fun and exciting. special events, discounts, giveaways – it’s never a dull moment. She is happy to help you with questions you may have regarding our products or services. Cat is a graduate of William & Mary, where she studied Government/Pre-Law and minored in Marketing.